|
International Journal of Bioelectromagnetism Vol. 6, No. 2, pp. 49-54, 2004. |
www.ijbem.org |
|
Altered Regional Restitution Properties Michiyasu Yamakia,
Tetsu Watanabeb, Koichi Yuukib, So Yamauchib,
Yukio Hosoyaa, aDivision of Medical informatics, and
bDivision of Cardiology, Pulmonology and Nephrology, Correspondence: M Yamaki. Division of Medical
informatics, Yamagata University School of Medicine, Abstract.
Background: The mechanisms of arrhythmogenicity in heart failure or myocardial
infarction remain poorly understood. We examined the relationships between
electrical abnormalities in restitution properties and ventricular arrhythmia
by using experimental and computer models. Methods: Sixty unipolar electrograms
were recorded from the entire cardiac surface in control dogs, pacing-induced
heart-failure dogs, and infracted dogs. The restitution properties and inducibility
of ventricular fibrillation (VF) were examined. Simulation studies using an Wei-Harumi
model were also performed. Results: In dogs with failing hearts, activation-recovery
intervals (ARI) were prolonged mainly at the apex. The slopes of the ARI restitution
curve in failing heats were significantly steeper than those in control hearts.
VF was easily induced by programmed stimulation in failing hearts, whereas no VF
occurred in control hearts. In dogs with chronic myocardial infarction, ARIs were
prolonged mainly at the anterior left ventricle. The ARI restitution slopes in
dogs with induced VF were significantly steeper than those without VF on anterior
left ventricle. Computer simulation studies could reproduce the experimental results.
Altering the ARI restitution to the steep slope causes VF in a model heart.
Conclusion: The steepness of regional electrical restitution may play an important
role in arrhythmogenicity in heart failure or myocardial infarction
Keywords: restitution; ventricular fibrillation; computer model; ischemia; heart failure 1. Introduction Ventricular arrhythmia is a significant contributor of sudden death in heart disease. Recently, the restitution mechanism has focused attention as the mechanism determining the transition of tachycardia to ventricular fibrillation [Riccio et al, 1999] [Weiss et al, 1999] [Garfinkel et al, 2000]. The restitution of electrical recovery represents the dynamic beat-to-beat relationship between diastolic interval (DI) and action potential duration (APD) on the heart. However, the role of restitution relationship on the ventricular fibrillation has not been established in injured in-vivo hearts, such as heart failure or myocardial infarction. The purposes of the present study are to investigate the role on the mechanism of dynamic changes in repolarization on the ventricular fibrillation in in-vivo hearts and computer simulation. The present study may provide information on the mechanism on the life threatening arrhythmia. 2. Material and Methods 2.1. Operation procedure Forty-two adult mongrel dogs were studied and divided into three subgroups; heart failure, myocardial infarction and control, according to the operation procedure. All dogs were anesthetized by intravenous administration of sodium pentobarbital (30 mg/kg body wt.), intubated, and ventilated with a constant-volume ventilator. ECG (lead II) was monitored continuously. In twenty-two dogs (heart failure group), a programmable pacemakers were implanted to introduce the pacing-induced heart failure by applying constant rapid heart rate (200 bpm) for 3 weeks. These dogs were allowed to fully recover from surgery for 7 days, after the rapid pacing. In twelve dogs (myocardial infarction group), left fifth intercostal space thoracotomy was performed and the pericardium was opened under aseptic conditions, then, left anterior descending coronary artery at the level just distal of its first diagonal branch was permanently occluded for 4 weeks. Another eight dogs that underwent sham operation skin incision left coronary were served as a control group. All dogs were treated with antibiotics for 2 weeks After the above procedure, all dogs were anesthetized again. The heart was exposed by thoracotomy and suspended in a pericardial cradle. Sinus node was crushed, and a bipolar stimulating electrode was attached to the right atrium. The heart was paced at a cycle length of 200-600 msec with 2 msec duration square-wave stimuli at twice diastolic threshold intensity. To maintain the temperature and humidity, thoracic cavity was covered with plastic wrap while recording the electrograms. A polyethylene catheter was placed into a femoral vein and physiological saline solution was infused at a constant rate. An arterial line was inserted into the right femoral artery to continuously monitor the mean arterial pressure. The electrocardiogram lead II and blood pressure were monitored throughout the study on a model 2G66 recorder (NEC San-Ei, Tokyo, Japan). Sixty silver wire unipolar electrodes attached to a nylon stocking that was stretched over the heart were used for recording cardiac surface electrograms. These electrodes were arranged into 10 columns. Each cardiac surface electrode was referenced to a Wilson's central terminal. Sixty-lead electrograms were recorded simultaneously with a sampling interval of 1 msec, by the use of CD-G015 system (Chunichi Denshi Co., Nagoya, Japan) [Konta et al, 1990] [Kubota et al, 1993]. 2.2. Data processing We calculated activation-recovery intervals (ARIs) and diastolic intervals (DIs) for each electrogram. ARI was defined as an interval between the minimal derivative in the QRS complex and the maximum derivative in T wave. ARI is known to be faithful measure with APD [Millar et al, 1985][Haws et al. 1990]. The relationship between ARIs and DIs was examined during atrial pacing with cycle lengths of 800 to 300 msec in step of 100 ms decrement and from 300 msec to the Wenckebach block in steps of 10 to 20 ms. The relationship between ARIs and DIs is shown in the following function; ARI = b(1- e-a·DI), to quantify them as an electrical restitution curve. Slopes of ARI restitution curve were measured for each epicardial lead. Susceptibility of ventricular arrhythmia was investigated by programmed stimulation. Ventricular effective refractory period was determined by use of a driving train (S1) of ten beats with a cycle length of 400 ms, followed by an extrastimulus (S2) that was decremented in 10-ms intervals. Ventricular effective refractory period was defined as the longest S1S2 interval at which S2 failed to elicit ventricular activation. The second extrastimulus (S3) was started with the S1S2 interval fixed at 40 ms longer than the ventricular effective refractory period. The S2S3 interval decrements until S3 failed to elicit ventricular activation. 2.3. Simulation studies The simulation study using a Wei-Harumi model was performed [Harumi et al,1989 ][Wei et al. 1995]. The heart model includes atria and ventricles and comprises 50,000 discrete units (model cells). The model cells were categorized into 8 types: sinus node, atria, atrioventricular node, bundle of His, bundle branch, Purkinje fiber, ventricular cells, and connective element. The electrophysiological properties of each model cell were specified as in previous reports [Yamaki et al. 1999] and were also specified as measurements in a representative pacing-induced heart failure model. Excitation automaticity was assigned only to sinus node cells. Other types of cells were activated from neighboring cells when those cells became excitable. When cells were absolutely refractory, conduction was completely blocked. The restitution slope (RS) on a simulation study was defined as the difference in APDs divided by the difference in CIs. This parameter yields APD change with CI and is uniquely determined for each cell type.
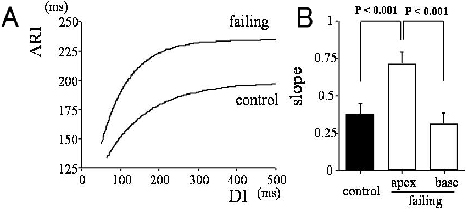
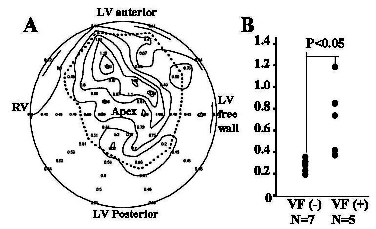
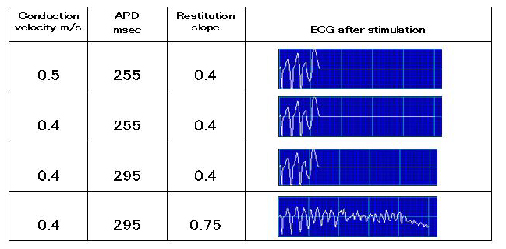
Trains of electrical stimuli were delivered to an anterior apex cell at a cycle-length of 160 msec. The heart model was considered to be located inside a homogeneous torso model. The surface potentials on the model torso generated by the heart model were calculated by means of the prescribed transmembrane action potential distribution d [Harumi et al,1989 ][Wei et al. 1995]. This simulation generates torso surface ECG, since we employed the boundary element method for calculation. 2.4. Statistical analysis Statistical inferences were made by use of SAS (Statistical Analysis System) program (SAS Institute Inc., Cary, NC). Data are expressed as mean ± standard deviation. Statistical significance was assessed by analysis of variance (ANOVA) with post hoc Bonferroni tests for multiple comparisons. A confidence level of 95% was considered statistically significant. section describes the format for figures, tables, equations and references. 3. Results 3.1. Heart failure The restitution relation between ARI and DI was examined at the apical and the basal myocardium. Figure 1A shows the representative ARI restitution curves in control and failing heart. In the representative curves, the slopes of the ARI restitution in failing hearts were steep at short diastolic interval, compared with control hearts. In figure1B, group difference in the maximal slopes between control (n = 6) and failing hearts (n = 6) were displayed. The slope of the ARI restitution curve at the apex of failing hearts was significantly steeper than that of control hearts. However, the slope of the ventricular base was almost equal to that of the control hearts. Programmed electrical stimulation was performed to examine arrhythmogenicity in failing hearts. Ventricular tachycardia (VT) was easily initiated by double extra-stimuli at a drive cycle length of 400 msec in all failing hearts (10/10 dogs), while no ventricular arrhythmia were initiated by the same extra-stimuli in control hearts (0/8 dogs). Induced VT in failing hearts degenerated into VF (9/10 episodes). Figure 1. R representative ARI restitution curves in control and failing heat A). Maximal slopes of the restitution curves in control (n = 6) and failing hearts (n = 6) on apical or basal myocardiu B). ARI;activation-recoveryinterval,DI;diastolic interval. 3.2. Myocardial infarction The dynamic restitution relation was investigated during constant atrial pacing in myocardial infarction dogs. The maximal slopes of the restitution curve were measured on each lead point of a cardiac surface. A representative trace of maximal slope of ARI restitution curves was displayed by an apical polar projection (Figure 2A). The map indicated that the slopes were steep in infarcted region, i.e. anterior wall. When we examined the difference in restitution slopes between VF(+) and VF(-) groups, the restitution slope in VF(+) myocardial-infarction dogs significantly increased on the anterior epicardium, compared with VF(-) group. The mean slope was 0.75in VF(+) dogs Figure 2. Representative trace of regional ARI restitution slopes in a case of myocadial infarction A), and slopes on a anterior lead in VF(-) and VF(+) groups. In pannel A, display format is apicalpolar projection. In farcted area was enclosed by dot line. The slopes in inafrcted area were steep. In pannel B, the slopes in VF(+) group were steeper than those in VF(-) group. RV; right ventricle, LV;left ventricle, VF;ventrcular fibrillation. 3.3. Myocardial infarction The simulation setups and results were displayed in figure 3. In the present study, we modified the following three parameters; 1) slow conduction, 2) prolonged APD and/or 3) an increase in restitution slope. As shown in figure 3, simulation results after four trains of stimulation indicated that VF continued only when greater restitution slope was applied. Increase in DC is essential for the induction of VF in the model heart Figure 3. Simulation setups and results. Increase in restitution slope is essential for the induction of VF in the model heart. APD; action potential duration. 4. Discussion 4.1. Main findings In the present study, we examined the relation between electrophysiological alterations and ventricular arrhythmia in heart failure and myocardial infarction. The results uggested that steepness of electrical restitution curve is important for arrhythmia vulnerability in heart failure. The simulation study verified that an increase in restitution slope was essential for the induction of VF. Altered electrical restitution properties may play an important role for arrhythmogenicity 4.2. Restitution hypothesis and electrical instability Recently, restitution properties have been focused on the transition between ventricular tachycardia and fibrillation (the restitution hypothesis) [Riccio et al, 1999] [Weiss et al, 1999] [Garfinkel et al, 2000]. In a case with steep slope of the restitution curve, small changes of diastolic interval, i.e. extra-stimuli, produced a larger change in the action potential duration of the next beat. The larger the action potential duration changes, the larger the diastolic interval changes. Therefore, alteration in the action potential duration and diastolic interval was augmented, and finally VF occurred. Riccio et al. reported that a steep slope of the electrical restitution curve was a prerequisite for VF and reduction of the restitution slope prevented the development of VF [Riccio et al, 1999]. We thought simulation studies using a model is an important process for linking the hypothesis to the observed phenomena. Therefore, we constructed the three-dimensional heart model simulating injured-heart electrophysiology. The simulation results also showed that increase in restitution slope was essential for VF. It confirmed the importance of restitution hypothesis on the mechanism of VF in injured hearts, such as heart failure or myocardial infarction. 4.3. Restitution slope and VF It is suggested that a slope over 1 of restitution relation facilitates the induction of APD alternans. [Riccio et al, 1999] In the present study, mean steepness of ARI restitution slope was 0.74 at apex in failing heart and 0.75 at infarct region in myocardial ischemia. However, VF was induced by ventricular extra-stimuli. The possible speculations are as follows; 1) the difference in pacing method; ventricular or atrial pacing. The atrial pacing is appropriate when investigating the injured hearts electrophysiology. However, the slopes measured with atrial pacing become dull than those with ventricular pacing, because of applicable short cycle length. 2) The provoked dispersion in recovery may directly cause the wave break of the electrical excitation, and 3) the conduction delay may affect on the dynamic relationships. To determine the precise mechanism about this point, the further studies will be needed. Conversely, in the control studies with normal restitution slope, VF was not induced. It suggests that the steep slope of ARI-DI relationship might be the substrate of ventricular arrhythmia even when it was below 1. 5. Conclusions The steepness of regional electrical restitution may play an important role in arrhythmogenicity in heart failure or myocardial infarction. The approach for controlling arrhythmia based on the restitution hypothesis may provide new insights into the antiarrhythmic strategy in patients with cardiac disease Acknowledgements This work was supported by the Research Grant for Cardiovascular Diseases (15-6) from the ministry of Health, Labor and Welfare, and The 21st Century COE Program from the Ministry of Education, Science, Sports, and Culture of Japan (Molecular Epidemiological Study Utilizing the Regional Characteristics). References
Harumi, K., H. Tsunakawa, G. Nishiyama, D. Wei, G. Yamada, Y. Okamoto and T. Musha. Clinical application of electrocardiographic computer model. J. Electrocardiol. 22(Suppl): 54-63, 1989. Haws CW, Lux RL. Correlation between in vivo transmembrane action potential durations and activation-recovery intervals from electrograms. Effects of interventions that alter repolarization time. Circulation , 81(1):: 281-8, 1990 Garfinkel A, Kim YH, Voroshilovsky O, et al. Preventing ventricular fibrillation by flattening cardiac restitution. Proc Natl Acad Sci USA , 97(11): 6061-6, 2000 Konta T, Ikeda K, Yamaki Y, Nakamura K, Honma K, Kubota I, YasuiS. Significance of discordant ST alternans in ventricular fibrillation. Circulation , 82(6): 2185-89,1990. Kubota I, Yamaki M, Shibata T, Ikeno E, Hosoya Y, Tomoike,H . Role of ATP-sensitive K+ channel on ECG ST segment elevation during a bout of myocardial ischemia. A study on epicardial mapping in dogs. Circulation , 88(4): 1845-51,1993 Millar CK, Kralios FA, Lux RL. Correlation between refractory periods and activation-recovery intervals from electrograms: effects of rate and adrenergic interventions. Circulation , 72(6): 1372-9, 1985 Riccio ML, Koller ML, Gilmour RF Jr. Electrical restitution and spatiotemporal organization during ventricular fibrillation. Circ Res,84(8); 955-6,1999 Watanabe T, Yamaki M, Yamauchi S, Minamihaba O, Miyashita T, Kubota I, Tomoike H. Regional prolongation of ARI and altered restitution properties cause ventricular arrhythmia in heart failure. Am J Physiol , 282(1): H212-8.,2002 Wei D, Okazaki O, Harumi K, Harasawa E, Hosaka H. Comparative simulation of excitation and body surface electrocardiogram with isotropic and anisotropic computer heart models. Ieee Transactions on Biomedical Engineering 42(4): 343-357, 1995 Weiss JN, Garfinkel A, Karagueuzian HS, Qu Z, Chen PS. Chaos and the transition to ventricular fibrillation: a new approach to antiarrhythmic drug evaluation. Circulation , 99 (21): 2819-26,1999 Yamaki, M., I. Kubota and H. Tomoike. Simulation of late potentials and arrhythmias by use of a three-dimensional heart model: casuality of peri-infarctional slow conduction in ventricular fibrillation. J. Electrocardiol., 32(2): 115-121, 1999 Yuuki K, Hosoya Y, Kubota I, Yamaki M. Dynamic and not static change in ventricular repolarization is a substrate of ventricular arrhythmia on chronic ischemic myocardium.Cardiovasc Res, 63(4):645-52,2004
|