|
International Journal of Bioelectromagnetism Vol. 6, No. 2, pp. 41-48, 2004. |
www.ijbem.org |
|
Derivation of Respiratory Signal from Single- Shuxue Dingab, Xin Zhua, Wenxi Chena, Daming Weia Correspondence: S Ding, Department of Computer Software, The University of Aizu, Tsuruga, Ikki-machi, Abstract.
Respiration derivation from ECG signals would be an alternative approach for
obtaining respiration related knowledge that is especially useful in the situation
in which the respiration is not routinely monitored by specialized equipment.
Although several published methods could give reasonable results for this purpose,
for some applications, they still have drawbacks in some respects, e.g., requiring
multi-channel ECG signal, being robust-less against noise, etc.. In order to overcome
these drawbacks, in this paper, we investigate the possibility of obtaining respiratory
knowledge from a single-channel ECG signal based on its higher order statistics,
which is a notable feature that the conventional methods do not hold. Another
worthy of mention feature is that the method depends on R-wave detections only,
such that other feature detections, e.g., Q-wave or S-wave detection, are not
necessary anymore for the processing. This feature does not make the processing
simpler only, with the feature related to higher order statistics together, but
it also strengthens the robustness against noise. Our experiments show the
improved performances with the method.
Keywords: Derived Respiration; ECG; Respiratory Signal; Higher order statistics; Single-Channel.
1. Introduction The ECG-derived respiration is the respiratory signal, or say, the respiratory knowledge that is derived from ECG signals. This is especially important in the case that the ECG, but not the respiration, is routinely monitored. One can perform respiratory signal extractions by some signal processing approaches. There have been several efforts for such a purpose [Moody, Mark and Zoccola, 1985, Moody, Mark and Bump, 1986, Lipsitz, Hashimoto, Lubowsky, Mietus, Moody, Appenzeller, Goldberger, 1995, Nazeran, Behbehani, Yen and Ray, 1998, and Behbehani, Vijendra, Burk, Lucas, 2002]. These methods are based on the facts that 1) the positions of ECG electrodes on the chest surface move relative to the heart, and 2) transthoracic impedance varies, as the lungs fill and empty, during the recording of the ECG. An existent method is used to take advantage of the fact 1) or both of the fact 1) and the fact 2). For performing such a method, multi-channel ECG signal are usually required. If the method invokes only the fact 1), the ECG signal of precordial leads is required either. Some methods that are based on filtering or wavelet have been proposed [Yi, Park, 2002]. However, such a method has not been shown theoretically underlain, since as shown in the next section, the respiration acts as a modulation on, rather than an additive signal to, the ECG source. In some situations, one might have only a single-channel ECG signal. Furthermore, this signal might not be from one of the precordial leads. This is the case especially for some ECG monitors for non-professional use. In such a situation the conventional approaches do not work. In this paper, we resolve this problem and propose an approach for respiratory extraction from a single-channel that is not necessarily from a precordial lead. One of the most notable features of our proposed approach is that it invokes the higher order statistics of ECG recording such as the 4-th order cumulant. Just because of this, we can perform a respiration extraction from a single and non-precordial lead. In contrast to this, the conventional approach usually employs the geometric quantities of some ECG characteristic waves, e.g., QRS complex. Besides of requiring signals of precordial multi-leads, another drawback of such a method is that, besides of the R-wave detections, it needs Q-wave and S-wave detections as well. Since these waves are usually low valued, or say, have low signal-to-noise ratios (SNRs), comparing to that of the R-wave, the method trends less robust against noise. Considering employing the higher order statistics, it might be worthy for us to compare this approach with so the called independent component analysis (ICA) [Cichocki and Amari]. This technique is for the purpose of blind source separation (BSS) that sounds similar to that of this paper. Indeed, there existed several research works for applications of ICA on ECG sources [Cardoso, 1998]. ICA is also usually performed based on higher order statistics. Although ICA can also be used for the source extraction, it is not a good tool for the present purpose. The reason is, as discussed in Section 2, the ECG source is modulated by the respiration, instead of being superposed by a respiration source, as in a case that the ICA applicable. The approach proposed in this paper is as follows. First, we remove the baseline wandering. Second, we detect the R-waves. Third, we calculate the kurtosis between each two neighboring R peaks, from which we derive a respiratory strength at the RR periodic. After this, we spline the samples and filter the signal to obtain the smoothed respiratory signal. In Section 2 we give the problem description and the proposed method. We also discuss the theoretical properties of the proposed method. In Section 3, we evaluate the performance with some numerical results via a public ECG bench marker with monitored respirations. In Section 4, we give discussions and draw conclusions. 2. The Method 2.1 The Problem Description The basic problem is briefly described. It is assumed that an ECG source that is usually generated inside the heart of human. This source is unknown and transferred in a linear medium leading to an ECG sensor signal u(t) instant t that may include an underlying signal v(t) , i.e., a baseline drift, and an additive sensor noise n(t),
where A(t) denotes the transfer characteristic of the linear medium from the ECG source to the sensor. Usually, it is either positive definite or negative definite. In this paper, without losing generality, we assume that it is positive definite. The transfer characteristic acts as a modulation on the ECG source. Usually, the additive sensor noise is approximately Gaussian distributed. Medically, several leads of ECG signals are recorded in different places. u(t) can be considered as one of the leads. Since, in most situations, the linear medium is the human body, this transfer characteristic should be mainly related to a variation of the body conditions. One of the important variations of the body conditions is an impedance variation of body, or say, the thorax, due to the respiration. The underlying signal, i.e., baseline drift v(t) is generated due to the variation of interaction between the sensor and the body. One of the variations of interaction is the electrical resistance variation between the sensor and the skin. Of course there may be other kinds of variation factors. However, the most important two factors should be the respiratory modulation and the baseline drift. Therefore, we obtain
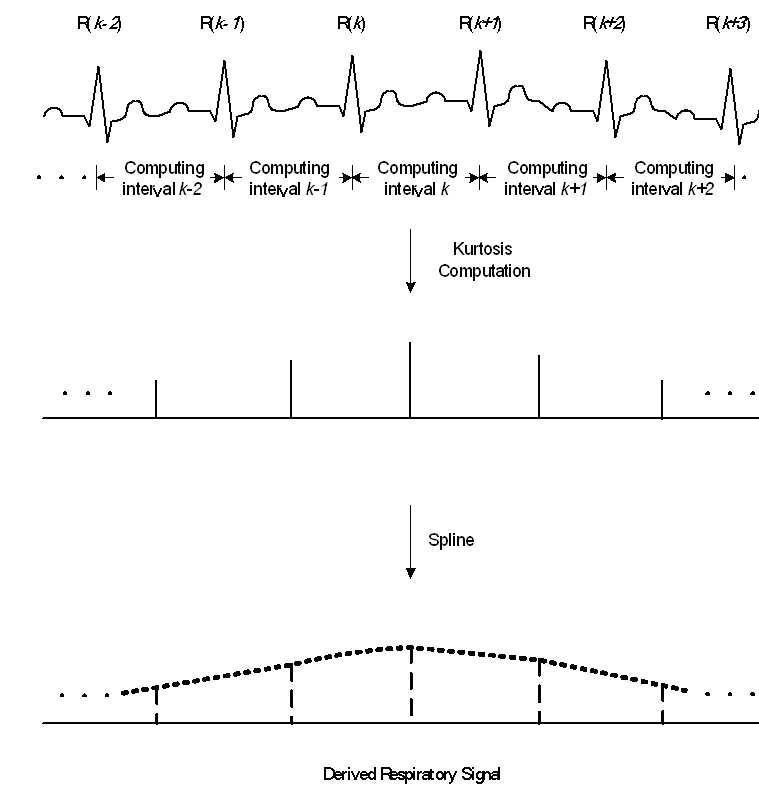
if the other modulation factors are so small that can be neglected. Here, I(t) denotes the transfer characteristic part of the thorax impedance. The problem concerned about in this paper is how to derive a respiratory signal, which is related to I(t), from the ECG signal u(t). This is possible because that the variation of I(t) is much slower than that of s(t) . Before we can do this, removing the baseline drift is required, since it is not of our interest and might affect the quality of the derived respiration. 2.2 The Method and Its Theoretical Principle In this paper, we propose a method for deriving respiration, which invokes the higher order statistics of a single-channel ECG signal. The steps and the block diagram for the signal processing are shown in Fig.1 and Fig. 2, respectively. As the first step, we perform the removal of baseline drift in the recorded ECG signal. This can be done based on some differences between the baseline drift and the ECG source. These differences include, 1) the baseline drift and the ECG source are independently generated, 2) the baseline drift is random but an ECG usually has some special patterns, 3) in most situations, the frequency of baseline wander is much lower than the appearing frequency of QRS complex [Raifel and Ron, 1997]. In this paper, we employ the down-sampling and up-sampling method [Ifeachor and Jervis, 1993]. After this processing, we obtain the baseline wander removed ECG signal
The second step performs R-wave detections. We employ the first derivative method [Pan and Tompkins]. We assume there are totally R-waves in the period we are considering, and we have detected R-waves that are at samples with numbers tk for k=1,2,...N. Here k denotes the number of each R-wave. The detected value of R-peak at k-th R-wave is x(tk). Figure 1. Steps for signal processing of the respiratory extraction. Figure 2. Block diagram for signal processing of the respiratory extraction. The third step performs the 4-th order cumulant, i.e., the kurtosis, computations in each interval of two neighboring R-waves, as shown in Fig. 1.
where
In deriving this equation, the noise is assumed to have zero mean
and zero skewness,
Since the ECG source s(t) is unknown for us, its value for
and
where γ and σ are constant. In facts, σ2 is the variance and γ4 is the 4-th variance for s(t) in the interval of the sample number from tk to tk+1-1. Substituting Eqs. 6 and 7 into Eq. 5, we obtain
where
Since, usually, I(t) is much more slowly variant comparing to the RR interval,
which is the interval for the expectation calculation, we may suppose
it to be constant approximately in each RR interval, i.e., .
From Eq. 9, if the kurtosis value between each RR interval is known, we may obtain the respiratory sample at the k-th R-wave as
This equation shows the theoretical principle of respiration derivation based on the higher order statistics of the ECG signal. In other words, given the kurtosis value of the recorded ECG signal between two neighboring R-waves, we can estimate a respiratory source sample for the RR-interval. Though this sample can be assigned to any one ECG signal sample between two neighboring R peaks, in this paper, it is assigned to the former R peak. In such a way, we can obtain each respiratory source sample at R peak, and a time series of these samples forms the estimated respiratory waveform. Once having obtained
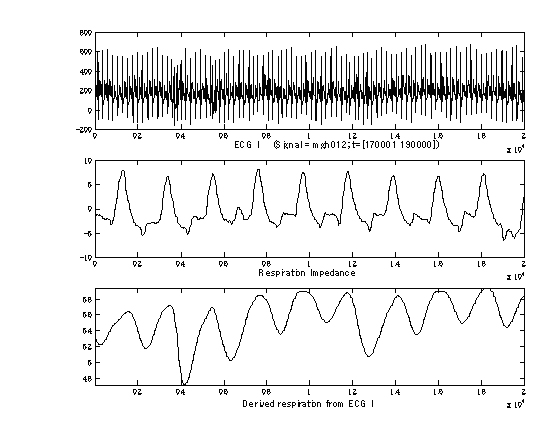
2.3 The Theoretical Features of the Proposed Method There are three important properties for the proposed method. First, although there exist several characteristic waveforms in ECG, e.g., P-, Q-, R-, S-, and T-waves, the proposed method is related to the R-waves only. This property benefits the method with a high accurate respiratory signal and a strengthened robustness against noise. This is due to that usually an R-wave is much higher valued and has a higher SNR, comparing with that of other waves, which are weaker with poorer SNRs. Therefore, it is less erroneous to estimate R-waves. Second, the method is of statistics dependent. Therefore, it is not sensitive to variety in the ECG structures. Third, the respiration is related to both the lower-order statistics and the 4th-order statistics of the signal. It can be proved that the method depends on the whole-order statistics as well, if it depends on the 4th-order statistics. In other words, this method will invoke full statistics of the signal. It can also be proved that, if the additive noise is Gaussian distributed, it will not affect our estimation results, since its kurtosis equals to zero. 3. Results A sample plot of ECG signal, measured respiration and derived respiration is shown in Fig. 3. The upper panel plots the original ECG I signal. The middle panel plots the recorded respiration via the impedance measure. The lower panel plots the derived respiration with the proposed method. As can be seen from this plot, the derived result is generated as a continuous waveform reflecting the respiration.
Figure 3. The ECG I signal (top), the respiration impedance (middle) and the derived respiration Tab. 1 shows evaluation results with the MGH/MF waveform database in PhysioNet [Goldberger et al., 2000]. We chose ten data, and each data contains both the ECG I signal and the respiration impedance signal. We derived the respiration with the proposed approach. The respiration impedance was taken as a reference signal for evaluation. For a quantitative evaluation, we compare the respiratory counts in the respiration impedance with that in the derived respiration, in the same time interval. We give the relative accuracy rate, with the respiratory count by the respiration impedance as the reference. From the table, there was no significant difference between the two counts. Note that we chose some specified intervals where the impedance respiration for the reference had clearer waveform for easier comparing with the derived respiration. By experiments, in most other intervals or with most other data, we could also obtain very similar waveforms for derived respirations to that in the specified intervals shown in Fig. 3. Table 1. Evaluation results with the MGH/MF waveform database in PhysioNet [Goldberger et al., 2000].
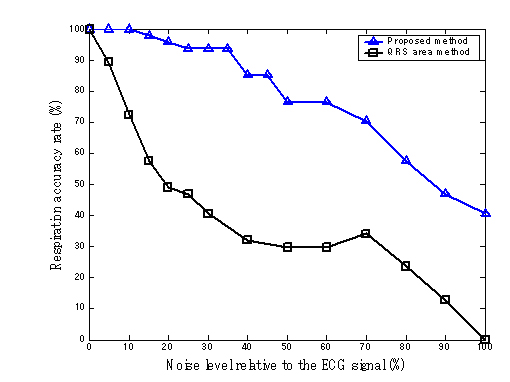
Figure 4. The accuracy rate versus the noise level Fig. 4 plots the results of the respiration count accuracy rate versus the noise level. This is for evaluate the robustness of the proposed method against the noise, in contrast to a conventional approach - QRS complex area method [Moody, Mark, Zoccola and Mantero, 1985]. The noise is additive Gaussian. The results agree with the theoretical expectation that the propose approach has a higher robustness. The figure shows a much greater robustness of the proposed method than that of the conventional method, even though the proposed method use only a single-channel of ECG, while the conventional method uses two-channel of ECGs. Note that when the noise level equals to the ECG signal level, the conventional method cannot work at all since the accuracy rate is zero. However, even in such a situation, the proposed method can still work to some extent. There are two reasons for this phenomenon. First, the proposed algorithm needs only R-wave detections, where the SNRs are high enough even though the overall signal average energy equal to the noise average energy, while the conventional method needs the detections of Q-and S-wave as well, where the SNRs are poorer. Second, in the proposed algorithm, the kurtosis is used for deriving the respiration, which is hardly affected by the additive Gaussian noise, while the QRS complex area is used in the conventional method, which is greatly affected by the additive Gaussian noise. 4. Conclusions In this paper, we proposed a method for the respiration extraction from a single-channel ECG signal. The method invoked the higher order statistics of the signals, in contrast to the conventional methods that used only geometric characteristics of feature waves and the lower-order statistics. We also gave the theoretical derivation that showed the principle possibility. With the MGH/MF waveform database in PhysioNet database, our evaluations showed better respiration accuracy rates, and a more powerful robustness against the additive Gaussian noise than that of the conventional method. One of the reasons was that the proposed method needed only R-wave detections where SNRs were higher comparing with other waves. Another reason was that the respiration was derived based on the kurtosis of the signal, which was hardly affected by the additive Gaussian noise. Since the proposed method is effective even for a single-channel ECG, it is expected applications in some specialized ECG monitors. Acknowledgements This work was supported in part by the project No. 16500134, 2004 Grants-In-Aid for Scientific Research, Ministry of Education, Culture, Sports, Science and Technology, Japan. This work was also supported in part by the funding from University Start-Ups Creation Support System of the Japanese Ministry of Education, Culture, Sports, Science and Technology (MEXT). References
Behbehani K, Vijendra S, Burk JR, Lucas EA. An investigation of the mean electrical axis and respiration during sleep. In proceedings of the Second Joint EMBS/BMES Conference. 2002, 1550-1551. Cardoso JF, Multidimensional independent component analysis. In proceedings of ICASSP'98. 1998, 1941-1944. Cichocki A, Amari S. Adaptive Blind Signal and Image Processing. John Wiley & Sons, LTD., 2003. Ifeachor EC, Jervis BW. Digital Signal Processing - A Practical Approach. Addison-Wesley Publishing Company, Wokingham, England, 1993, 492-505. Lipsitz LA, Hashimoto F, Lubowsky LP, Mietus J, Moody GB, Appenzeller O, Goldberger AL. Heart rate and respiratory rhythm dynamics on ascent to high altitude. British Heart Journal 74(4):390-396, 1995. Moody GB, Mark RG, Zoccola A, Mantero S. Derivation of respiratory signals from multi-lead ECGs. Computers in Cardiology, 12: 113-116, 1985. Moody GB, Mark R, Bump M. Clinical validation of the ECG-derived respiration (EDR) technique. Computers in Cardiology, 13: 507-510, 1986. Nazeran H, Behbehani K, Yen FC, Ray R. Reconstruction of respiratory patterns from electrocardiographic signals. In proceeding of the 2nd International Conference on Bioelectromagnetism, 1998, 183-184. Pan J, Tompkins WJ. A real-time QRS detection algorithm. IEEE Transactions on Biomedical , 32(3): 230-236, 1985. Raifel M, Ron S. Estimation of slowly changing components of physiological signals. IEEE Transactions on Biomedical Engineering, 44(3): 215-221, 1997. Yi WJ, Park KS. Derivation of respiration from ECG measured wothout subject's awareness using wavelet transform. In proceeding of the Second Joint EMBS/BMES Conference. 2002, 130-131. Goldberger AL, Amaral LAN, Glass L, Hausdorff JM, Ivanov PCh, Mark RG, Mietus JE, Moody GB, Peng CK, Stanley HE. PhysioBank, PhysioToolkit, and PhysioNet: Components of a New Research Resource for Complex Physiologic Signals. Circulation 101(23):e215-e220 [Circulation Electronic Pages; http://circ.ahajournals.org/cgi/content/full/101/23/e215]; 2000 (June 13).
|