|
International Journal of Bioelectromagnetism Vol. 6, No. 1, pp. 58-62, 2004. |
www.ijbem.org |
|
Non-Invasive Electrical Imaging of Heart: N.K. Suresh Kumar and M.Ramasubba Reddy Indian Institute of Technology, Madras, India Correspondence: N.K. Suresh Kumar, Biomedical Engineering Division, Indian Institute of Technology Madras, Chennai 600036, India. Abstract. The objective of this
work is to develop a technique to make non-invasive electrical imaging of heart
(NEIH), as a routine clinical practice. NEIH gives the electrical activity of
Heart by reconstructing maps of Epicardial potentials from measured body surface
potentials. The accuracy of the reconstructed maps depends on Inverse method and
the Forward solution. The effects of homogeneity and geometrical modeling errors
on the computed forward solution are studied. Two cases are considered with four
geometrical models. Forward solution is computed by Finite Element Method using
SCIRun. In the first case forward solutions of a homogenous and an inhomogeneous
geometrical model of similar geometrical size are studied. In the second case
forward solutions of two inhomogeneous geometrical models with same torso size
but with different heart size (systolic and diastolic conditions) are studied.
The results show that in the first case the potential pattern remained the same
with change in magnitude only. In the second case both the potential pattern and
magnitude are changed. Geometrical error in the model has adverse affects on the
forward solution. These studies suggest that a dynamic and patient specific
geometrical model is required for exact computation of forward solution. For
reconstruction in terms of isopotential maps, homogenous Patient Specific Model
will serve better, than inhomogeneous Non-Patient Specific Model. A new method
is suggested as a solution for patient specific model, in which Heart surface is
constructed from ultrasound image of Heart and Body surface by photographic method
Keywords: Electrical Imaging of Heart, Epicardial Potential Reconstruction, Forward Problem, Patient Specific Model
1. Introduction The spatial information content of the electrical activity of the heart increases considerably by reconstructing potential maps on the surface of the heart (Epicardium) [Brooks and MacLeod, 1994]. Various Inverse methods exist to solve this. All of these methods require a model of volume conductor which adequately describes the relation between the potentials on the Epicardial surface and the Body surface potentials [Gulrajani, 1998]. The creation of a high quality model is a complex procedure. To use this technique in clinical environment further increases the complexity as individual patient specific model is needed. Also size of the heart varies continually throughout the cardiac cycle. Therefore the level of details needed to be included in the geometric model is to be analyzed. The level of details of the two most important aspects of the simulation, the conductivity values assigned to each region of the geometry and the geometry of the thorax itself is still an important research topic. In this work the effect of modeling errors due to conductivity and geometry of the thorax is evaluated. The results can serve as a guide for selecting appropriate model to be used in the electrical imaging of heart. 2. Methods: This section describes the formulation of the forward problem and the numerical simulations performed. 2.1 Forward Problem: Electrocardiographic forward problem in terms of epicardial sources is represented as
Where
Equation (1) along with (2) and (3) was solved by Finite Element Method. Finite element model for solving the above equation was constructed from the surface mesh data. Two unstructured triangular surface meshes were considered, the body surface mesh and the heart surface mesh with 790 and 128 number of nodes respectively. The surface mesh data was available with SCIRun Dataset [SCIRun,2002]. Tetrahedral mesh was generated within the volume bounded by the above mentioned surfaces using the mesh generation software TetGen. Tetrahedra were chosen because of their ability to approximate the irregular surfaces of the human body and because they are well suited to fully automatic mesh generation algorithms [MacLeod et al., 1991; Johnson et al., 1991]. As a part of the tetrahedralization procedure, each element also received a group number based on the tissue type assigned to the cell. This group number later served as the means of flexibly assigning conductivity values to each element in the model [Klepfer et al., 1997]. 2.2 Simulations: A common network for computing the body surface potentials from the assumed heart surface potentials was created and solved using SCIRun. Simulations were carried for two modeling errors. Effect of Conductivity Error: First, the effect of modeling error due to conductivity assigned for a region (homogeneous and inhomogeneous), was studied. For this a low resolution model with 938 nodes and a high resolution model with 168,000 nodes with different geometries were used. The conductivity values assigned for the low resolution inhomogeneous model was 0.68s/m for the heart region and 0.2s/m for the region in between heart and body surfaces [Klepfer et al., 1997]. The high resolution model was the Utah Torso model available with SCIRunDataset[SCIRun,2002]. The Boundary condition (Heart Surface Potentials) assumed for low resolution model was one time instant of the potentials recorded over the canine heart with 128 sock electrodes , the same set of potentials were interpolated over the heart surface of high resolution model. Forward solutions were computed for all the models [Shahidi et al., 1994; Gulrajani , 1997 ]. Effect of Geometrical Error: In the second type of simulation, the effect of Geometrical modeling error was studied. Geometric error was simulated by scaling only the heart surface mesh, while keeping the body surface mesh unaltered. Then tetrahedral mesh was constructed from these two surface meshes. The scaling was done by varying the heart size linearly. Three models were constructed with +10%, 5%, 2% change in the heart size. Forward solutions were computed for both reference model and scaled models. 3. Results: Simulation results were evaluated qualitatively by comparing the maps constructed from the potentials of nodes only on the body surface [MacLeod, 1993]
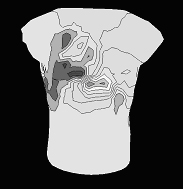
Figure 1. The body surface potential map for first simulation (effect of conductivity) with a low resolution model; figure 1 (a) is the potential map for homogenous model and figure 1(b) is the potential map for inhomogenous model.
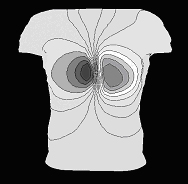
Figure 2.The body surface potential map for first simulation (effect of conductivity) with a high resolution model; figure 2 (a) is the potential map for homogenous model and figure 2(b) is the potential map for inhomogenous model.
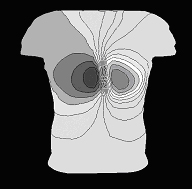
Figure 3.shows the body surface potential map for second simulation (variation in geometry); figure 3 (a) is the potential map for the reference model and figure 3(b) is the potential map for the model whose heart size is increased by 2% from the reference model.
Figure 4.The body surface potential map for second simulation (variation in geometry); figure 4 (a) is the potential map for the reference model and figure 4(b) is the potential map for the model whose heart size is increased by 5% from the reference model.
Figure 5.The body surface potential map for second simulation (variation in geometry); figure 5 (a) is the potential map for the reference model and figure 5(b) is the potential map for the model whose heart size is increased by 10% from the reference model. 4. Discussion The results show that in the first case the potential pattern remained the same with change in magnitude only. In the second case both the potential pattern and magnitude are changed. For 2% change in heart size the change in potential pattern was less, but in 5% change pattern change became significant .The pattern changed completely for 10% change in heart size. The 10% change in size could be considered as a geometrical error due to Non-Patient specific model. Hence Geometrical error in the model has adverse affects on the forward solution, which in turn determines the accuracy of the Inverse solutions. The 2% and 5% change in sizes could be considered as a geometrical error due to change in heart size from systole to diastole. This adds to the requirement of dynamic heart model. As the potential pattern remains the same for both homogeneous and inhomogeneous model one can opt for simple homogeneous model. Also, as there is variation in both pattern and magnitude for variation in the geometry size, dynamic and patient specific model only will give accurate inverse epicardial potential reconstructions. 5. Conclusion For reconstruction in terms of isopotential maps, homogenous Patient Specific Model will serve better, than inhomogeneous Non-Patient Specific Model. A new method is suggested as a solution for patient specific model, in which Heart surface is constructed from ultrasound image of Heart and Body surface by photographic method. References
Bronzino JD: Biomedical Engineering Handbook, CRC Press, 1999. Brooks DH and MacLeod RS: Imaging the electrical activity of the heart: direct and inverse approaches, Proceedings. ICIP-94., IEEE International Conference, 3,548-552, 1994. Gulrajani RM: The forward and inverse problems of electrocardiography, IEEE Engineering in Medicine and Biology, September/October, 84-101, 1998. Gulrajani RM: The forward problem of electrocardiography: from heart models to body surface potentials, Proceedings of the 19th Annual International Conference of the IEEE, 6, 2604 -2609,1997. Johnson CR and MacLeod RS; Computer models for calculating transthoracic current flow, Proceedings of the Annual International Conference of the IEEE,13,768-769,1991. Klepfer RN, Johnson CR and MacLeod RS: The Effects of inhomogeneities and anisotropies on electrocardiographic fields: a three-dimensional finite element study, IEEE Trans. Biomedical Eng., 44, 706-719,1997. MacLeod RS, Johnson CR and Ershler PR: Construction of an inhomogeneous model of the human torso for use in computational electrocardiography, Proceedings of the Annual International Conference of the IEEE,13,688-689,1991. MacLeod RS and Johnson CR: Map3d: Interactive scientific visualization for bioengineering data. In IEEE Engineering in Medicine and Biology Society 15th Annual International Conference, pages 30-31, IEEE Press, 1993 Malmivuo J and Plonsey R: Bioelectromagnetism, Oxford University Press, New York, 1995. Plonsey R: Bioelectric Phenomena, McGraw-Hill Book Company, New York, 1969. SCIRun: A Scientific Computing Problem Solving Environment. Scientific Computing and Imaging Institute (SCI), http://software.sci.utah.edu/scirun.html, 2002. Shahidi AV, Savard P and Nadeau R: Forward and inverse problems of electrocardiography: modeling and recovery of epicardial potentials in humans, IEEE Trans. Biomedical Eng., 41,249-256, 1994.
|