|
International Journal of Bioelectromagnetism Vol. 5, No. 1, pp. 53-56, 2003. |
www.ijbem.org |
|
Electrical Impedance and Cardiac
Monitoring — Mart Mina, Stig Ollmarb, Eberhard Gersingc aInstitute of Electronics, Tallinn
Technical University, Tallinn, Estonia Correspondence: M. Min, Institute of Electronics,
Tallinn Technical University, 19086 Tallinn, Estonia. Abstract. Alterations
in electrical properties of tissues, detectable by non-invasive or
minimally invasive electrical impedance measurements and signal processing,
carry information about organ function and tissue state. Cardiac applications
include cardiac output, timing patterns and ischemia. Measurements
are fast, cheap, and harmless, and may replace other techniques in
some proven diagnostic or monitoring applications, while adding useful
complementary information to others.
Keywords: Impedance Cardiography; Intracardiac Bioimpedance; Electrical Impedance Spectroscopy; Ischaemia 1. Background All physiological or pathological phenomena are intrinsically bioelectrical or accompanied, directly or indirectly, by changes in electrical properties of the tissue or organ under test. Thus, it is likely that measurements of electrical parameters would serve well to characterize or estimate most events or conditions in the human body, provided that the desired information can be distinguished from a huge number of simultaneously occurring processes. In cases where inherent biopotentials such as ECG or EEG are used, distance to the source (i.e. body surface recording or direct contact with the organ) is an anatomical parameter determining the signal level and its correlation with the properties of the organ. From an engineering point of view, the signal could be enhanced by amplification and filtering or more advanced methods of signal processing, as well as selecting a place with a low level of EMI from the environment. If dielectric properties are used to extract information, electrical energy of one or several frequencies is supplied to the tissue under test (Fig.1a), and the signal to noise ratio can be greatly enhanced using synchronous detection principles. Although superior data quality will be achieved using electrodes in direct contact with the tissue under test, one has still to consider that surrounding tissues will be involved to some degree, and the degree of parasitic information will depend on the exact placement of the electrode system and the actual distribution of dielectric parameters, as well as the dynamic size and shape of the body or body section. The fundamental theory behind dielectric (impedance) methods is well understood (Fig.1b) and published [Foster and Schwan, 1989; Grimnes and Martinsen, 2000], the remaining challenges concern adaptation and optimization of the technique for specific applications.
Figure 1. Tissue under test with the current flow paths through the cell structure (a), and frequency spectrum of the dielectric permittivity ε and corresponding dependance of capacitive reactance XC (b). 2. Material and Methods 2.1. Some Target Applications of Electrical Impedance Measurement (EIM) Among the relatively established applications of EIM are body composition analysis [Lukaski, 1987; Cornish, 1993; Thomas, 1998], Electrical Impedance Tomography [Metherall at al., 1996; Holder et al., 1999; Smallwood at al., 1999; Patterson et al., 2001], and alterations in skin and oral mucosa [Nicander et al., 1996; Rantanen et al., 2002; Nicander et al., 2003; Åberg et al., 2003].
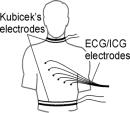
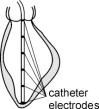
Figure 2. Electrical bioimpedance cardiography: noninvasive plethysmography (a), multielectrode invasive estimation of the ventricular volume (b), intracardiac impedance based pacing control (c and d). Cardiac applications have been focused at estimating cardiac output, using non-invasive [Kubicek et al., 1966], see Fig.2a, or invasive [Baan et al., 1981] technique (Fig.2b). Further developments and clarifications have been contributed by several researchers [Baura, 2002], e.g. by taking into use the ECG electrodes for concurrent ICG measurement [Kauppinen et al., 1999], and see ECG/ICG electrodes in Fig.2a. The invasive ICG was taken into use in 1980s [Baan et al., 1981], see Fig.2b, and has been applied in cardiac pacemakers [Salo, 2002; Webster, 1995]. The ICG application has not been a story of permanent success. The noninvasive ICG was formally approved for full Medicare coverage in the USA only in September 1998 [Baura, 2002]. Other recent intracardiac measurements include using very thin catheter or pacemaker electrodes [Ericsson et al., 2001; Söderqvist et al., 2001; Järverud et al., 2002], and monitoring of myocardium ischemia [Gersing, 1998; Schaefer et al., 2002] or myocardium energy balance [Kink et al., 2000], see Fig.2c and 2d. 2.2. Bioimpedance Measurement Nowadays bioimpedance applications of multielectrode systems (Fig.2) require multiplexed measurements at several frequencies from the audio range up to tens of MHz (multipoint impedance spectroscopy), [Osypka and Gersing, 1994; Kauppinen et al., 1999; Min et al, 1999, 2002], see Fig.3. A distortion free and near to real-time extraction of impedance variations, or two-phase (0º and 90º) synchronous demodulation of the real (Re) and imaginary (Im) parts of biomodulation (Fig.3) of cardiac impedance due to heart beating and respiration (Fig.2d), is the aim of measurement [Grimnes and Martinsen, 2000; Min et al., 2000].
The multichannel generation of multi-frequency excitations simultaneously is a means to reduce the number of needed switchings in the multiplexer and to obtain reliable results during a short measurement cycle. Generation of the simultaneous multi-frequency excitation requires application of digital waveform synthesizers and, unfortunately, also a far better signal resolution and a more complicated signal processing of response signals. Only about 16- to 20-bit digitizing resolution and sophisticated digital signal processing (DSP) means can ensure demodulation of every frequency component of the multifrequency response separately and practically simultaneously for getting near to real-time presentation [Min et al., 1999]. 2.3. Detection of Ischemia Caused Cardiac Tissue Deterioration by Impedance Spectroscopy With the interruption of the blood supply to organs (ischemia), oxygen and substrates rich in energy are no longer delivered to the tissue and the metabolic products are no longer removed. The tissue is increasingly injured and finally damaged to such an extent that viability goes lost. Because tissue structures (extra- and intracellular compartments, membranes) affect the electric current conduction (Fig.1a), measurements of tissue impedance spectra (Fig.1b) during ischemia will reflect the progressive deterioration of the tissue and determine reliably when the organ runs into the critical range before the irreversible loss of life. In the following example impedance spectroscopic measurements in myocardial tissue during ischemia (animal experiment, for details see Gersing, 1998) is presented. After isolation from the circulation, the heart muscle has been perfused with a cold cardioplegic solution for 8 minutes in order to slow down the injurious processes in tissue. For impedance measurements an excised sample was incubated in a temperature controlled chamber at 25°C.  Fig.4 shows the relative changes in conductance at 100 Hz and 10 MHz during ischemia and the course of the contraction index, a measure of the contraction of the muscle cells caused by deficiency in energy (rigor mortis). At high frequency the conductance increases almost linearly up to about 300 minutes, at low frequency after about 150 minutes the conductance decreases rapidly to a lower plateau (260 minutes). At that time muscle cells start to contract. Conductance at high frequency is a measure of the total amount of mobile ions in the tissue, which increases as long as the metabolism is active, i.e. up to 300 minutes. Conductance (real part of admittance) at low frequency (reflecting the extracellular compartment, the conductance of the cell membranes and the state of the gap junctions) shows a rapid decrease after 150 minutes indicating closing gap junctions [Kehrer et al., 1990]. When they are closed the contracture begins. 3. Discussion and Conclusions The result of ischemia studies shows that an organ can be successfully resuscitated up to the decline of the conductance at low frequency. Later on, resuscitation will be possible with an increasing time for recreation, but after the closure of the gap junctions' revivability is normally lost. From the results it can be concluded, that impedance spectroscopy is an appropriate method (and harmless to the tissue) for determining the state of organs during ischemia. ([Schaefer et al., 2002], with a comprehensive list of references). The impedance measurement at several frequencies simultaneously widens perspectives of cardiac monitoring in vivo. Although one might instinctively prefer non-invasive implementations of the technology, this should not limit creativity and applications. Clearly, in several applications invasive electrode systems do not add to the degree of invasiveness inferred by other medical actions, e.g. intracardiac catheters for pressure measurements or pacemaker electrodes. One might therefore predict further development in the direction of getting as close as possible to the signal source in order to obtain highest quality data for diagnose/characterization of tissue alteration or monitoring of cardiac function, without the non-invasive limitation/restriction. On the other hand, non-invasive technologies for cheap and simple monitoring of vital parameters will have its applications, although there will always be a risk of confounding data unless verified by other methods. Acknowledgements This work was supported by Estonian Science Foundation, grant no. 4859, the Karolinska Institute, Sweden, St. Jude Medical AB, USA-Sweden, and Deutsche Forschungsgemeinschaft. References Åberg P, Nicander I, Holmgren U, Geladi P, Ollmar S. Assessment of skin lesions and skin cancer using simple electrical impedance indices. Skin Res Technol, 2003 (in press). Anderson FA. Impedance plethysmography, in Encyclopedia of Medical Devices and Instrumentation. Webster JG, Editor. John Wiley & Sons, New York, 1988, 111-122. Baan J, Jong TTA, Kerkhof PLM, Moene RJ, van Dijk AD, van der Welde ET, Koops J. Continuous stroke volume and cardiac output from intra-ventricular dimensions obtained with impedance catheter. Cardiovasc Res, 15: 328-334, 1981. Baura G. System Theory and Practical Applications of Biomedical Signals, Ch. 6: Improved Impedance Cardiography. IEEE Press, Wiley, New Jersey, 2002. Cornish BH, Thomas BJ, Ward LC. Improved prediction of extracellular and total body water using impedance loci generated by multiple frequency bioelectrical impedance analysis. Phys Med Biol, 38: 337-346, 1993. Ericsson AB, Kronander H, Söderqvist E, Vaage J, Brodin LÅ. Correlation between a mid-ventricular volume segment and global left ventricular volume measured by the conductance catheter. Scand Cardiovasc J, 35: 129-135, 2001. Foster KR, Schwan HP. Dielectric properties of tissues and biological materials: A critical review. Crit Rev Biomed Eng, 17: 25-104, 1989. Gersing E: Impedance spectroscopy on living tissue for determination of the state of organs. Bioelectrochemistry and Bioenergetics, 45: 145-149, 1998. Grimnes S, Martinsen ØG. Bioimpedance & Bioelectricity Basics. Academic Press, London 2000. Holder DS, Gonzalez-Correa CA, Tidswell T, Gibson A, Cusick G, Bayford RH. Assessment and calibration of a low-frequency system for electrical impedance tomography (EIT), optimised for use in imaging brain function in ambulant human subjects. Ann NY Acad Sci, 873: 512-519, 1999. Järverud K, Ollmar S. Brodin LÅ. Analysis of the O-wave in acute right ventricular apex impedance measurements with a standard pacing lead in animals. Med Biol Eng Comput, 40: 512-519, 2002. Kauppinen PK, Hyttinen JAK, Kööbi T, Malmivuo J. Multiple lead recordings improve accuracy of bio-impedance plethysmographic technique. Medical Engineering & Physics, 21(5): 371-375, 1999. Kehrer G, Aminalai A, Gersing E, Lamesch P, Meissner A, Schareck WD, Richter J, Bretschneider HJ: Glycogen effects on energy state and passive electric properties of liver during protection. Z Gastroenterol. 28: 147-156, 1990. Kink A, Min M, Parve T. A Rate Adaptive Pacemaker. Int. publ. No. PCT WO 00/57953 and WO 00/57954, 2000. Kubicek WG, Karnegis JN, Patterson RP, Witsoe DA, Mattson RH. Development and evaluation of an impedance cardiac output system. Aerospace Med, 1208-1212, 1966. Lukaski HC. Methods for the assessment of human body composition. Amer J Clin Nutr, 46: 537-556, 1987. Metherall P, Barber DC, Smallwood RH, Brown BH. Three-dimensional electrical impedance tomography. Nature, 380: 509-512, 1996. Min M, Parve T, Kukk V, Kuhlberg A. An Implantable Analyzer of Bio-Impedance Dynamics: Mixed Signal Approach. IEEE Trans. on Instrum. & Measurement, 51(4): 674-678, August 2002. Min M. Electrical Bioimpedance Measurement: The Means and methods for Applying in Cardiac Monitoring and Pacing. In: proc. of the 1st World Congress on Biomimetics and Artificial Muscles, Albuquerque, New Mexico, Dec 2002, 6 p. Min M, Märtens O, Parve T. Lock-in Measurement of Bio-Impedance Variations. Measurement, 27(1): 21-28, 2000. Min M, Märtens O, Parve T. Multisine dynamic EBI spectrum analyser for in vivo experiments. Medical & Biological Engineering & Computing, 37, 1999, Suppl.2, Part I, Proc. of the European Medical and Biological Engineering Conf. EMBEC'99, Wien, Austria, Nov 1999, 144-145. Nicander I, Ollmar S, Lundh-Rozell B, Eek A, Emtestam L. Correlation of impedance response patterns to histological findings in irritant skin reactions induced by various surfactants. Br J Dermatol, 134: 221-228, 1996. Nicander I, Rantanen I, Lundh-Rozell B, Söderling E, Ollmar S. The ability of betaine to reduce the irritating effects of detergents assessed visually, histologically and by bioengineering methods. Skin Res Technol, 9: 50-58, 2003. Patterson RP, Zhang J, Mason LI, Jerosh-Herold M. Variability in the cardiac EIT image as a function of electrode position, lung volume and body position. Physiol Meas, 22: 159-166, 2001. Rantanen I, Nicander I, Jutila K, Ollmar S, Tenovuo J, Söderling E. Betaine reduces the irritating effect of sodium lauryl sulphate on human oral mucosa in vivo. Acta Odontol Scand, 60: 306-310, 2002. Salo R. Experience with the PRECEPT Impedance Controlled Pacemaker. In proc. of the 1st World Congress on Biomimetics and Artificial Muscles, Albuquerque, New Mexico, Dec 2002. Schaefer M, Gross W, Ackemann J, Gebhard MM: The complex dielectric spectrum of heart tissue during ischemia, Bioelectrochemistry, 58: 171-180, 2002. Smallwood RH, Hampsire AR, Brown BH, Primhak RA, Marven S, Nopp P. A comparison of neonatal and adult lung impedances derived from EIT images. Physiol Meas, 20: 401-413, 1999. Söderqvist E, Carlsson C, Brodin LÅ, Elmqvist H, Kronander H, Ericsson AB. Design of a single segment conductance catheter for measurement of left ventricular volume. In proc IEEE-EMBC, Istanbul, Oct 2001, 25-28. Thomas BJ, Ward LC, Cornish BH. Bioimpedance spectrometry in the determination of body water compartments: accuracy and clinical significance. Appl Radiat Isot, 49: 447-455, 1998. Webster GJ. Design of Cardiac Pacemakers. IEEE Press, New Jersey 1995.
© International Society for Bioelectromagnetism
|