|
International Journal of Bioelectromagnetism Vol. 5, No. 1, pp. 80-83, 2003. |
www.ijbem.org |
|
First 36-Channel System for Clinical
Magnetocardiography in Unshielded Hospital Laboratory for Riccardo Fenicia,
Donarella Brisindaa, Anna M Melonia, Peter Fenicia aClinical Physiology - Biomagnetism Research
Center, Catholic University of Sacred Heart, Correspondence: R Fenici Clinical Physiology - Biomagnetism Research Center, Catholic University of Sacred Heart, L.A. Gemelli 8, 00168 Rome, Italy. E-mail: feniciri@rm.unicatt.it, phone +39 06 3051193, fax +39 06 3051343 Abstract. Multichannel Magnetocardiography
(MMCG) is a contactless method, which provides non-invasive three-dimensional
imaging of cardiac electrogenetic phenomena. However a multichannel system
reliable in an unshielded hospital environment was needed, to bring it into
clinical practice. We have recently installed the first 36-channel system
for MMCG operating in an unshielded EP catheterization laboratory, and validated
its accuracy for cardiac source localization. In this paper an overview is
given of system performance during daily clinical use. The 36-channel recording
lasts typically 90 seconds. Post-processing takes 2 minutes. A standard bicycle-ergometer
protocol has been used for exercise MMCG. Equivalent current dipole (ECD),
Effective Magnetic Dipole (EMD) and distributed currents (DC) models are used
for 3D source localization and multimodal imaging. Since November 2002, 256
patients, affected by different kinds of cardiac problems, were studied at
least twice to test for reproducibility. The new system is fully reliable
and provides 3D source localization as well as quantitative estimate of electrophysiological
parameters, with accuracy good enough for clinical use.
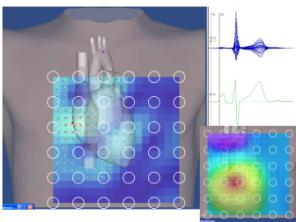
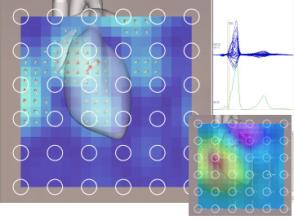
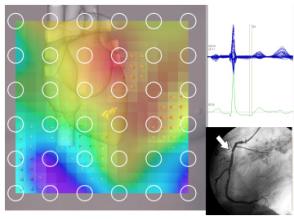
Keywords: Magnetocardiography; Ischemic Heart Disease; Cardiomyopathy; Ventricular Repolarization; Multimodal Cardiac Imaging; Cardiac Arrhythmias; Cardiac Electrophysiology; Monophasic Action Potential 1. Introduction 40 years have passed since the first human magnetocardiogram was recorded [Baule and Mc Fee, 1963]. Since then, much research work has been done in the field of "Magnetocardiography", and the number of multichannel MCG equipments and hospital installations is increasing. However, with a Medline query, only 136 clinical articles can be found at the moment [http://www.ncbi.nlm.nih.gov/PubMed/, 2003]. This is probably due to the fact that most of the research and even clinical work is still confined in magnetically shielded rooms (MSR) and performed by non medical scientists, cooperating with a limited number of clinicians. Therefore, in spite of its strong potentiality, as a functional imaging method for non-invasive study of cardiac electrophysiology, MMCG has not yet achieved the rank of a routine clinical tool. With this in mind, we have worked to develop, and recently installed, the first "user-friendly" multichannel system, with the unique ability to operate in an "unshielded" intensive care and cardiac electrophysiology laboratory. In this paper we will share the results of our preliminary experience with such instrumentation. 2. Material and Methods The multichannel instrumentation (CardioMag Imaging Inc, USA) (CMI) is a 36-channel system, based on LT-DC-SQUID sensors, coupled to second-order axial gradiometers (baseline: 55 mm), measuring the z-component of local magnetic fields simultaneously at 36 positions in a plane, from a 20 cm x 20 cm square grid. Intrinsic sensitivity of measuring channels in the factory low-noise open environment is typically better than 20 fT/√Hz at 1 Hz. The cylindrical cryostat is mounted in a way that it does not interfere with the operational capability of the cardiologist during invasive electrophysiological interventions (See Fig. 1). Figure 1. Biomagnetism and Cardiac Electrophysiology Laboratory, at the Catholic University. The MCG system is efficient even in relatively close proximity with modern digital fluoroscopy. In the insert: typical noise spectrum of one recording channel (bandwidth: DC-100 Hz). Recording bandwidth is typically DC -100 Hz (or 500 Hz). Standard data acquisition lasts typically 90 seconds. Windows NT-based data acquisition provides 24 bits A/D conversion, at 1-4 KHz sampling frequency. Post-processing of MCG signals is performed with CMI Windows NT-based PC software. For additional analysis, the same set of MCG data are also exported to an HP 735 UNIX workstation and analyzed with other software packages (Neuromag, Finland). Since November 2002, 256 patients, with different cardiac abnormalities (ischemic heart disease (IHD), cardiomyopathy, paroxysmal atrial arrhythmias, ventricular preexcitation, ventricular arrhythmias) have been investigated, at least twice, to test for reproducibility. Furthermore, a protocol has been developed, for stress-MCG, which is performed in our ambulatory patients, during standard 12-lead ECG effort test, carried out with a conventional bicycle ergometer [Fenici et al., 2002]. The source localization accuracy of the new multichannel system has been tested with our standardized amagnetic catheter technique in a phantom filled with saline [Fenici et al., 2003]. 3. Results During the installation of the 36-channel mapping system, it was confirmed that "radiofrequency" (RF) is the major problem, which might impede the reliability of MMCG in unshielded hospitals of a modern town [Fenici et al., 2001]. However, as for the previous 9-channel, this problem was overcome with adequate technological interventions, and the 36-channel system is fully operating, with average sensitivity of 20 fT/ÖHz or better, in the frequency range of interest for clinical MCG (1 to 100 Hz), even during rush hours (see Fig. 1). Digital filtering of the 50 Hz noise was necessary to detect cardiac signals in real time. After digital filtering, the P wave was appreciable on a beat-to-beat sequence in the majority of patients. However time averaging was necessary to image and to localize weak magnetic fields generated by atrial activity. After time averaging, typically of 90 seconds, the quality of the signals was good enough for magnetic field reconstruction and three-dimensional source localization (see Fig. 2). The uncertainty of 3D localization of an artificial current dipole embedded in the tip of the amagnetic catheter placed in a phantom filled with saline, ranged between 5 and 10 mm, with high reproducibility [Fenici et al., 2003]. The average time required to obtain 3D localization of the distal terminal of the amagnetic catheter was less than 3 minutes, from the start of data acquisition. In 38 patients with ventricular preexcitation (VPX), MCG classification of VPX was certain in 35/38 pts (92.1%) and uncertain in 3/38 pts, with complex activation patters during the delta wave, suggesting multiple accessory pathways, which were unpredictable with ECG only (see Fig. 3). Figure 2. Example of source localization and current reconstruction, during right atrial depolarization. 3D imaging based on MCG data properly visualize the activation of the right atrium. Figure 3. Example right accessory pathway localization, in a patient with ventricular preexcitation. In 20 patients, with IHD documented by abnormal coronary angiography, quantitative analysis of MCG was effective in detecting abnormalities of ventricular repolarization, with sensitivity and positive predictive value above 90% [Brisinda et al., 2003] (see Fig. 4). Figure 4. Example of abnormal ventricular repolarization, in a patient with single-vessel disease. 4. Discussion Non-invasive MCG localization and imaging of electrophysiological phenomena is nowadays recognized and deserving increasing attention of clinicians [Carre et al, 2002; Tavarozzi et al, 2002]. However major limitations for widespread clinical use of MCG are the cost of the equipments and the need of electromagnetic shielding. In this study we present the preliminary results obtained with a novel multichannel instrumentation, reliable in an unshielded hospital laboratory, therefore at patient bedside. With this 36-channel system, 3D source localization accuracy was good enough for clinical use, and slightly better than that obtained with the 9-channel system [Fenici et al., 2003]. In patients, the new system provided faster non-invasive localization of VPX, which, compared to ECG, was more accurate to classify, non-invasively, complex paraseptal VPX and to identify multiple accessory pathways. Previous studies in MSR have shown that MCG is highly sensitive in detecting ventricular repolarization abnormalities in patients with chronic IHD [Hänninen et al., 2000; Kanzaki et al., 2003]. With our 36-channel, we had similar results without shielding. Furthermore we demonstrated that exercise-MCG is feasible, with a conventional ergometer, simultaneously with 12-lead ECG recording. MCG seems to provide high sensitivity to detect ventricular repolarization abnormalities due to exercise-induced myocardial ischemia, in patients with suspected IHD. However, further work is needed, on a larger patients population, to define better algorithm for ST-T automatic analysis. In fact, present accuracy of the methods used for quantitative analysis of ventricular repolarization after effort, might be affected by several factors: for instance, by proper selection of the baseline. Moreover the specificity of MMCG to differentiate ventricular repolarization abnormalities due to myocardial ischemia from those due to other cardiomyopathy [Korhonen et al., 2001] has not been defined yet. Finally, signal averaged MCG provided a clear-cut differentiation between atrial depolarization and repolarization, during the P wave. Interestingly such MCG parameters might be independent predictors of recurrences of paroxysmal atrial arrhythmias. Acknowledgements Supported by MIUR grants # 9906571299_001 and 2001064829_001. The authors are also grateful to C. Rosner. A. Bakarev, A. Braginski, N. Korsun, K. Sternickel and J. Poliakov for scientific cooperation and continuous support and update of the CMI system. The ongoing cooperation with J. Nenonen and M. Mäkijärvi of the Helsinki University is fundamental for us. The dedication of Mrs. V. Iacobini, our professional nurse, is outstanding and invaluable. References Baule GM, McFee R. Detection of the magnetic field of the Heart. Am Heart J, 66-96, 1963. http://www.ncbi.nlm.nih.gov/PubMed/, 2003 Fenici R, Brisinda D, Nenonen D, Makijarvi M, Fenici P. Study of ventricular repolarization in patients with myocardial ischemia, using unshielded multichannel magnetocardiography. In Nowak H, Haueisen J, Giebler F, Huonker R: Proceedings of the 13th International Conference on Biomagnetism. 2002: 537-539. Fenici R, Brisinda D, Nenonen J, Fenici P. Phantom validation of multichannel magnetocardiography source localization. PACE, 26 (Part II), 2003 (in press). Fenici RR, Brisinda D, Nenonen J, Morana G, Fenici P. First MCG multichannel instrumentation operating in an unshielded hospital laboratory for multimodal cardiac electrophysiology. Preliminary experience. Biomedizinische Technik, Band 46 (2): 219-222, 2001. Brisinda D, Meloni AM, Fenici R. First 36-channel magnetocardiographic study of CAD patients in an unshielded laboratoy for interventional and intensive cardiac care. FIMH 2003 (in press). Carre F, Painvin I, Poiseau E, Mabo P, Lessard Y, Daubert JC, Toulouse P. Magnetocardiography: principles and potential uses in cardiology. Arch Mal Coeur Vaiss, 95(10): 924-932, 2002. Tavarozzi I, Comani S, Del Gratta C, Di Luzio S, Romani GL, Gallina S, Zimarino M, Brisinda D, Fenici R, De Caterina R. Magnetocardiography: current status and perspectives. Part II: Clinical applications. Ital Heart J, 3(3): 151-165, 2002. Fenici R, Brisinda D, Nenonen J, Fenici P. Non invasive study of preexcitation by multichannel magnetocardiography. PACE, 26 (Part II), 2003 (in press). Hänninen H, Takala P, Mäkijärvi M, Montonen J, Korhonen P, Oikarinen L, Nenonen J, Katila T, Toivonen L. Detection of exercise induced myocardial ischemia by multichannel magnetocardiography in patients with single vessel coronary artery disease. Ann. Noninv Electrocardiology, 5: 147-157, 2000. Kanzaki H, Nakatani S, Kandori A, Tsukada K, Miyatake K. A new screening method to diagnose coronary artery disease using multichannel magnetocardiogram and simple exercise. Basic Res Cardiol, 98(2):124-132, 2003. Korhonen P, Vaananen H, Makijarvi M, Katila T, Toivonen L. Repolarization abnormalities detected by magnetocardiography in patients with dilated cardiomyopathy and ventricular arrhythmias. J Cardiovasc Electrophysiol, 12(7): 772-777, 2001.
© International Society for Bioelectromagnetism
|