 |
International Journal of Bioelectromagnetism Vol. 5, No. 1, pp. 72-75, 2003. |
www.ijbem.org |
|
Clinical Application of Magnetocardiography Jaakko Malmivuo and Juha Nousiainen Ragnar Granit Institute, Tampere University of Technology, Tampere, Finland Correspondence: J Malmivuo, Ragnar Granit Institute,
Tampere University of Technology, P.O. Box 692, FIN-33101 Tampere,
Finland. Abstract. The electric currents,
generated by the activating cardiac muscle, produce an electric field
on the surface of the skin recorded as electrocardiogram, ECG. The
same currents also induce a magnetic field in and around the thorax
recorded as magnetocardiogram, MCG. The main issue in applying MCG
is: Does the MCG include new diagnostic information, not present in
the ECG? It is shown that though the MCG leads are independent of
the ECG leads, the ECG and MCG signals are only partially independent.
The diagnostic performances of ECG and MCG are similar, but the groups
of patients they diagnose correctly, are not identical. Therefore,
when combining these methods to electromagnetocardiography, EMCG,
the diagnostic performance significantly increaes from that of the
ECG.
Keywords: Electrocardiogram; Magnetocardiogram; Diagnostic Performance 1. Introduction The tracings of the electric activity of the human heart, the electrocardiogram (ECG), were first measured in 1887 by Augustus Waller using capillary electrometer (Waller 1887). A pioneer in modern electrocardiography was Willem Einthoven who, at the beginning of the 20th century, developed the first high-quality ECG recorder based on the string galvanometer. In 1902 Willem Einthoven started clinical ECG. He summarized his results in ECG research in 1908 and 1913 (Einthoven, 1908; Einthoven et al., 1913). Since Einthoven's fundamental developments, electrocardiography has been the most important cardiac diagnostic method. The ECG signal is, due to its 1 mV amplitude, easily measurable on the surface of the thorax. Hans Christian Örsted discovered the connection between electricity and magnetism in 1819. The law of Biot-Savart states that electric current induces a magnetic field, which flows around the conductor of the current. This is, of course, true also for the bioelectric currents. When the cardiac cells activate, they generate a bioelectric current, which generates a bioelectric field, detected as electrocardiogram, ECG. Due to the law of Biot-Savart these bioelectric currents also induce a biomagnetic field, which is detected as magnetocardiogram, MCG. Thus, the MCG originates from the same phenomenon, as the ECG: from the depolarization and repolarization of cardiac cells. The first biomagnetic signal, the magnetocardiogram (MCG), was detected by Gerhard M. Baule and Richard McFee in 1963 with an induction coil magnetometer (Baule and McFee, 1963) Due to the basic laws of electromagnetism, the amplitude of the MCG signal is extremely low. Its amplitude is about one millionth of the earth's static field, being about 50 picoTeslas, and its successful measurement needs superconducting technology and a magnetically low-noise environment. After these 40 years of magnetocardiography, the technical difficulties in the instrumentation are now solved. The theory of bioelectromagnetic measurements and the relationship between ECG and MCG are finally understood. These fundamental accomplishments lay the basis for developing magnetocardiography a clinical tool. In this, and the following paper (Nousiainen et al, 2003), we describe the fundamental theory of magnetocardiography, how it should be applied to obtain clinically valuable results and prove this theory with a clinical study. 2. Independence of Bioelectric and Biomagnetic Signals The fundamental issue in biomagnetism is: Do the biomagnetic signals include information, not present in the bioelectric signals? If they do not, the only reason to apply magnetic measurement would be that the instrumentation does not need electrodes attached to the skin. The fundamental theorem discussing the independence of bioelectric and biomagnetic sources is the Helmholtz theorem which states: "A general vector field which vanishes at infinity, can be represented as a sum of two independent vector fields, one that is irrotational and another which is solenoidal." The cardiac electric source represented by the impressed current density J i form such vector field and due to Helmholtz theorem it may be divided to two components as follows: J i = J iF + J iV (1) These vector fields, J iF and J iV are referred to as flux source and vortex source, respectively. Bioelectric signals originate from the flux source and biomagnetic signals originate from the vortex source. Flux and vortex sources are general concepts, not concepts characteristic only to bioelectromagnetism. Robert Plonsey published in 1972 a paper (Plonsey 1972), which strongly stimulated the biomagnetic research. He claimed, on the basis of the Helmholtz theorem that "Since the flux and vortex sources are independent, ECG and MCG are similarly independent." If this had been the case, the MCG would include as much new independent information as the ECG already includes. Three years later, in 1975 Stanley Rush published a paper (Rush 1975), where he expressed a completely opposite view. He stated that: "The independence of the flow and vortex sources is only a mathematical possibility. The flow and vortex sources are one-to-one with each other." If a new lead is a linear combination of the existing leads, the information it gives from the source is a linear combination of the existing information and is not new, independent information. To obtain maximum amount of additional information from the source, such a lead must be used, which detects such component of the volume source, which is not detected by the existing leads. Assume that electrocardiogram is first detected with only one (dipolar) lead. This detects one component of the elementar electric sources. Another component of the elementar electric sources is detected by a lead, which is normal to the first one. This lead is independent on the previous one because one cannot construct it with a linear operation from the previous one. Even though these orthogonal leads detect orthogonal components of the source, the signals are not fully independent, because changes in the amplitude or angle of the source affect to both signals. In the rare occasion that only one component of the source changes, the signal changes only in that lead. This example demonstrates that even though two leads were independent, the signals, which they detect, are only partially independent. 3. Independence of Electrocardiogram and Magnetocardiogram The ECG and MCG are both generated by the bioelectric activity of the cardiac muscle. The ECG is a result of the flux source and the MCG is a result of the vortex source. What Helmholtz theorem states is, that the lead fields of the ECG and MCG are independent. In other words, the ECG and MCG leads are not linear combinations of each other. But as demonstrated above, the ECG and MCG signals are only partially independent. Thus, by recording the MCG, the diagnostic information obtained is only partially new. (Malmivuo and Plonsey, 1995) 4. Application of Magnetocardiography to Clinical Diagnosis According to Helmholtz theorem, a volume source is fully described if its flow and vortex sources are known. If we first work on dipolar level, this means that the dipolar electromagnetic source is fully described if its dipolar electric and magnetic sources are known. This means that we have to measure both vector electrocardiogram, VECG, and vector magnetocardiogram, VMCG. We call this combination vectorelectromagnetocardiogram, VEMCG. The three dipolar components of the VECG may be recorded with any appropriate vector (electro)cardiographic system, like Frank, axial, SVEC, or even with the 12-lead system, which mainly detects the dipolar cardiac source. The corresponding lead fields are illustrated in Figure 1.A. The three dipolar components of the VMCG may be similarly recorded with any appropriate vectormagnetocardiographic system like XYZ-, ABC-, or unipositional lead system. The corresponding lead fields are illustrated in Figure 1.B. These 3 + 3 = 6 electromagnetic dipolar signals are then fed to the computerized diagnostic system. It makes the diagnosis with just the same principle as diagnosis is traditionally made from the three electric dipolar signals. As it is described in detail in the next presentation (Nousiainen & al, 2003), the diagnostic performance of VMCG is similar to that of VECG. This is easy to understand because both methods have three dipolar leads and therefore detect similar amount of information from the cardiac source. But the patient groups, which these methods diagnose correctly, are not identical. This is a consequence from the fact, that the sensitivity distributions of these techniques are fundamentally different from each other. By using all the 6 dipolar electromagnetic signals as a VEMCG system, the diagnostic performance may be increased from either VECG or VMCG a statistically significant amount. This is indicated by decreasing of the number of incorrectly diagnosed patients to one half.
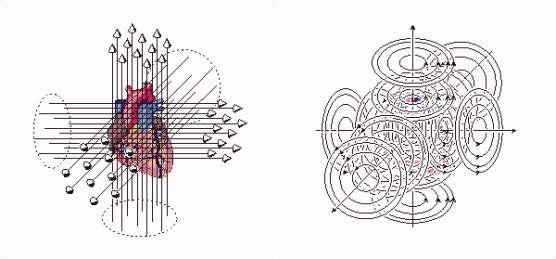 Figure 1. A ) The tree components of the ideal vectorelectrocardiographic lead system. B ) The three components of the ideal vectormagnetocardiographic lead system. 5. Recording of the Vectormagnetocardiogram In theory, the most straightforward method to record the VMCG is to make bipolar measurements of the magnetic source on the three coordinate axes. This is called the XYZ-lead system. For practical reasons this is not possible to realize. Some improvement may be achieved by rotating the coordinates to more symmetrical orientation as ABC-coordinates. The most practical way is to make the three orthogonal recordings in a single location above the heart. This is called the Unipositional lead system. The quality of the lead field is much improved if such recordings are made symmetrically on both sides of the thorax. (Malmivuo and Plonsey, 1995)
 Figure 2. A ) The XYZ-lead system. B ) The Unipositional lead system. References Baule GM, McFee R. Detection of the magnetic field of the heart. Am. Heart J. 55:(7) 95-6, 1963. Einthoven W. Weiteres über das Elektrokardiogram. Pflüger Arch. ges. Physiol. 122: 517-48, 1908. Einthoven W, Fahr G, de Waart A. über die Richtung und die Manifeste Grösse der Potentialschwankungen im mennschlichen Herzen und über den Einfluss der Herzlage auf die form des Elektrokardiogramms. Pflüger Arch. ges. Physiol. 150: 275-315, 1913. Malmivuo J, Plonsey R. Bioelectromagnetism - Principles and Applications of Bioelectric and Biomagnetic Fields. Oxford University Press. New York, 461 p. 1995. (Also: www.tut.fi/~malmivuo/bem/bembook) Nousiainen J, Malmivuo J, Oja O S. Combined Use of ECG and MCG in Classifying Myocardial Infarction. Int. J. Bioelectrom., 1, 2003. Plonsey R. Capability and limitations of electrocardiography and magnetocardiography. IEEE Trans. Biomed. Eng. BME-19:(3) 239-44, 1972. Rush S. On the interdependence of magnetic and electric body surface recordings. IEEE Trans. Biomed. Eng. BME-22: 157-67, 1975. Waller AD. A demonstration on man of electromotive changes accompanying the heart's beat. J. Physiol. (Lond.) 8: 229-34, 1887.
© International Society for Bioelectromagnetism
|

