|
International Journal of Bioelectromagnetism Vol. 5, No. 1, pp. 329-330, 2003. |
www.ijbem.org |
|
Dynamic Modeling of the Human Body
Jari Hyttinena,
Hanna-Greta Puurtinena, Pasi Kauppinena, Maria Pikkuhuhtaa,
aRagnar Granit Institute, Tampere University
of Technology, Tampere, Finland Correspondence: E-mail jari.hyttinen@tut.fi Abstract. Modeling of the dynamic properties
of the geometry related to the cardiac work may be of significant importance
in electrocardiogaphic studies. In impedance cardiography the signal originates
mostly from these changes. We have constructed two sets of dynamic models;
one based on image sets from systole and diastole and the other dynamic model
representing 18 time instants of the cardiac cycle. In both model sets the
volumes of more than 26 tissue types were determined. Single dipole simulations
of the cardiac sources indicate that the forward problem is affected considerable
by the change in geometry. However, the inverse localization of dipole source
is less vulnerable and the localization error is more due to matching of the
dipole location to the patients anatomy.
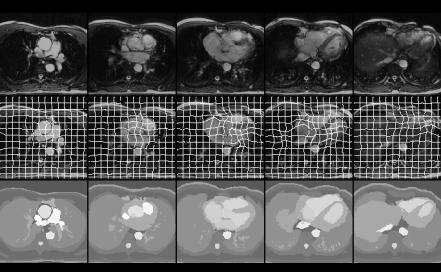
Keywords: Electrocardiography; Impedance Cardiography; Forward and Inverse Problem; Finite Difference Method 1. Introduction The shape and the inhomogeneities of the human thorax affect the electric field generated by the heart. Previously models of the thorax as a volume conductor have mainly been based on static sets of thorax images. The dynamic changes of the geometry due to the function of the heart may be of importance in ECG simulation and inverse problem. Likewise, the impedance cardiography is based on the measurement of the changes in the geometry and tissue impedance of the volume conductor affected by the heart function. The properties of the measurement systems can be estimated with static models [1], however, for the simulation of the impedance cardiography (ICG) signals a dynamic model is required. 2. Material and Methods We have constructed two sets of dynamic models of the thorax based on finite difference method (FDM). The first one is based on two MR image sets with 70 transverse slices presenting the anatomy during the diastole and systole. The data were segmented in order to construct two anatomically detailed models comprising of 228163 elements each. The models are identical except the geometry of the heart and large and some minor blood vessels. Altogether 26 distinct tissue types were segmented from the MR images using region growing type tools [1]. The body surface potentials of four dipole locations (X, Y and Z orientation) at different locations of the cardiac muscle were calculated. The dipoles were at the same location compared to the body surface in both models. Also the lead fields of the leads of the 120 channel body surface map system were calculated. The lead fields were obtained using the reciprocal current applied to the leads and the 120 calculations of each model provided the lead vectors in over 20 000 possible source nodes in the heart. In the inverse solutions these lead fields were used as forward solution to locate the simulated dipoles. The inverse solution was obtained firstly by using the same model for dipole and lead field calculation and then the lead fields obtained using different model than the simulated BSMs were used. Another dynamic model representing 18 time instants of the cardiac cycle was constructed. The high quality full thorax 56 slice cine MR images with 18 time frames were acquired with an ECG-gated, gradient echo sequence, with steady-state free precession. The resolution was 256x256 with field of view 46x46cm. Due to the relatively small size of the test person the region from the neck to below the heart was imaged. The images were segmented with a two-stage procedure. At the first stage the first timeframe (T=1) of the slice set was segmented using the semiautomatic region growing based tools. At the second stage a method based on deformable models [5] utilizing the segmentation result of the first time instant was used to segment the rest 17 phases. Fig. 1 demonstrates a segmentation result for this set at time step (T=5). In 1a) the transformed model and the original MR set are shown using a chess-board visualization technique. If the match was not good, it would be seen as discontinuous edges in the picture. These discontinuities are hardly visible in the result. The transformation is visualized in Fig. 2 by an elastic grid superimposed on the data along with the segmentation result. Figure1. Model 2; segmentation at time step T=5 at five different levels of the image stack. a) The transformed model and the original MR volume are shown using a chess-board visualization, b) the transformation is visualized by an elastic grid superimposed on the data. c) the resulting segmentation. 3. Results The results from model set 1 indicate that the forward solutions of the BSM generated by single dipoles are altered by the change of geometry of the heart and veins. The average RMS difference was 21% and 16%. There was a large variation in this effect depending on the dipole location. It ranged from less than 4 % (lateral left ventricle) to over 40% (septum). The inverse solution of the dipole locations was not affected by these changes and the location of the dipole was obtained correctly almost within the resolution of the FDM-model in the correct case and in the case when the lead fields and simulated BSMs were not from the same model. 4. Discussion Two FDM model sets have been constructed. The results from the model set 1 provide us initial knowledge regarding the effects of geometrical changes. The results are simulations without noise and the only change is the geometry of the model inhomogeneities during systole and diastole. According to the results the systole/diastole geometrical changes do not change the location of the inverse solution. Thus, the dipole location based on thorax outer surface remains stable even when wrong systole or diastole model is used. However, the location related to the cardiac muscle is changed. This means that the correct set of MR or other image data at the time instance corresponding to the BSM should be used even if the computational model is not dynamic. The new model set 2 with altogether 18 different time instances will provide the full dynamic properties of the geometry of the thorax. It will be applied for forward and inverse problem of electrocardiography and simulation of the impedance cardiography and tomography. References [1] Puurtinen H-G, Hyttinen J, Kauppinen P, ET AL. Including Anatomical Changes Due to Cardiac Function into a Model of a Human Thorax as Volume Conductor, Med. & Biol. Eng. & Comput., 1999; vol 37 Suppl 1: 234-235. [2] Lötjönen J. Segmentation of MR Images using Deformable Models: Application to Cardiac Images, IJBEM, 2001; Vol. 3, No. 2. (www.ijbem.org).
© International Society for Bioelectromagnetism
|