|
International Journal of Bioelectromagnetism Vol. 5, No. 1, pp. 104-105, 2003. |
www.ijbem.org |
|
Magnetocardiographic Alterations
Associated with Dirk Dunckera,
Illya Chaikovskyb, Elza van Deela, Robert van
Bremena, Michael Priminb,Monique de Waarda,
Paul Hugenholtza, Pieter Verdouwa, Edward McFallsa aExperimental Cardiology, Thoraxcenter,
Erasmus Medical Center, Rotterdam, The Netherlands Correspondence: I Chaikovsky, University Witten/Herdecke,
45134 Waldsaum1 Essen, Germany. Abstract. The aim of this
study was to determine whether global measures of MCG recordings collected
from anaesthetized swine correlate with changes in regional myocardial
function during graded regional ischemia and following ischemia-reperfusion
(stunning). 11 sedated swine (~25 kg) were transferred into the mobile
MCG unit, anaesthetized with pentobarbital and ventilated. 5 animals
were subjected to graded LAD flow reduction, 6 pigs underwent regional
flow reduction followed by reperfusion. MCG was recorded by means
of the 4-channel MCG system (MCG7, SQUID AG, Germany), installed in
an unshielded location. Every single current vector density map was
classified by one of the 5 classes (0 reflecting normal distribution,
4 reflecting highly pathological distribution). When regional segment
shortening (%SS) was plotted against the MCG Class during ischemia
an inverse relationship was observed that was highly significant (R=0.83;
P<0.01). The relationship between %SS following stunning and MCG
Class was less significant however (R=0.57; P=0.05).
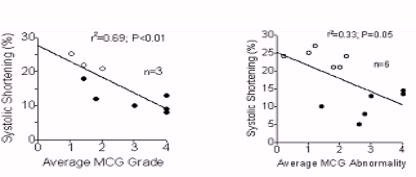
Keywords: Magnetocardiography; Myocardial Ischemia; Animal Experiments; Reperfusion 1. Introduction Magnetocardiography (MCG) has been proposed as a new non-invasive sensitive method for detection of myocardial ischemia. Although the technology has been applied to cardiac studies for nearly four decades, recent developments in protection from external non-cardiac sources as well as improved spatial resolution have generated renewed interest among investigators. Several small clinical trials have recently suggested that MCG recordings is more sensitive than the 12-lead resting and stress ECG for the detection of ischemia among patients with stable coronary artery disease. Nevertheless, an experimental confirmation of empirical findings is still pending. The objective of the present study was to correlate surface MCG changes with regional myocardial function abnormalities during variable levels of ischemia and following reperfusion. The anaesthetized open-chest swine model was used to determine accurate changes in regional function. 2. Material and Methods 11-crossbred Land race x Yorkshire pigs of either sex (n=10, 20-24 kg) were sedated with ketamine i.m. (20-30 mg kg-1, Apharmo, Huizen, The Netherlands), anaesthetized with sodium pentobarbital i.v. (20 mg kg-1, Sanofi, Paris, France), intubated and connected to a respirator for intermittent positive pressure ventilation with a mixture (1:2 vol%) of oxygen and nitrogen. Arterial blood gas values were kept within the normal range by adjusting respiratory rate and tidal volume. After administration of pancuronium bromide (4 mg, Organo Technique, So, The Netherlands) a midsternal thoracotomy was performed and the heart suspended in a pericardial cradle. The left anterior descending coronary artery (LAD) was dissected free just distal to the first diagonal branch for placement of a balloon occluder for later occlusion of the coronary artery. Regional wall function was measured using sonomicrometry (Triton Technology Inc., San Diego, CA, USA) by placing one pair of crystals in the distribution area of the LAD and one pair in the distribution area of the left circumflex coronary artery (LCx). After a 30 min stabilization period, baseline data of haemodynamics and regional myocardial function were recorded, and a magnetocardiogram was obtained. Animals were then randomised to one of two protocols. In the first protocol, the LAD was completely occluded for 15 min and reperfused for 2 hours. This protocol results in reversible myocardial dysfunction, i.e. stunning. In the second protocol, the LAD was partially occluded to result in variable degrees of loss of regional wall motion (mild-moderate hypokinesia), after which the coronary artery pressure was maintained constant. This protocol results in regional myocardial dysfunction without causing necrosis. All segment length data were normalized to an end-diastolic length (EDL) of 10 mm at baseline to correct for variability in the implantation distance between two crystals. Systolic shortening (SS) was computed as 100% x (EDL-ESL)/EDL, in which EDL and ESL (end-systolic length) are the segment length at the onset of the QRS complex and at the end of ejection (T wave), respectively. MCG was recorded by means of the 4-channel MCG system (MCG7, SQUID AG, Germany), installed in an unshielded setting in moveable trailer. MCG - examinations were performed at initial state and at every stage of occlusion and reperfusion based on the magnetic field distribution 20 subsequent current vectors maps were reconstructed with equidistant time step within the ST-T interval. Every single map was classified by one of the 5 classes (0 reflecting normal distribution, 4 reflecting highly pathological distribution). The classification is mainly based on the dipolar or non-dipolar structure of the map and the direction of the main current density vectors. The symmetry or asymmetry of the current vortices served for further specification. In other words, this classification is intended to evaluate the homogeneity of electrical properties of myocardium. Subsequently, 5 maps encompassing 40-65 % of the repolarisation interval were analyzed. This period was arbitrarily chosen to maximize predictive accuracy of the MCG changes for detection of ischemia. 4. Results In initial open-chest conditions majority of MCG maps remained Class 1 and sometimes 2. In 7 animals subjected to graded LAD blood flow reductions abnormalities in MCG maps became more severe, with Class 4 changes noted in 100% of the maps during complete LAD occlusion. Likewise, in 6 pigs that underwent regional LAD flow reduction followed by reperfusion (stunning) the majority of MCG maps demonstrated either Class 3 or Class 4 changes. In the three animals in which two consecutive variable degrees of stenosis were studied regional segment shortening (%SS) was plotted against the MCG Class during ischemia an inverse relationship was observed that was highly significant with R=0.83 and P<0.01 (see Fig1). The relationship between %SS following stunning and MCG Class was less significant however R=0.57 and P=0.05 (see Fig.2).
4. Discussion In open chest swine subjected to regional ischemia-reperfusion, MCG changes are noted at a time that regional myocardial function during and following ischemia-reperfusion is reduced. The severity of MCG abnormalities was most correlative with the reductions in regional function during ischemia and less correlative to the reductions in regional function following stunning
© International Society for Bioelectromagnetism
|